Pharmacotherapeutic group: Aminosalicyclic acid and similar agents.
ATC code: A07E C02.
Pharmacology: Pharmacodynamics: Mechanism of action: Mesalazine is an aminosalicylate. The mechanism of action of mesalazine is not fully understood, but appears to have a topical anti-inflammatory effect on the colonic epithelial cells. Mucosal production of arachidonic acid metabolites, both through the cyclooxygenase and lipoxygenase pathways, is increased in patients with chronic inflammatory bowel disease, and it is possible that mesalazine diminishes inflammation by blocking cyclooxygenase and inhibiting prostaglandin production in the colon. Mesalazine has the potential to inhibit the activation of nuclear factor kappa B (NFкB) and consequently the production of key proinflammatory cytokines. More recently, it has been proposed that impairment of PPAR-γ nuclear receptors, (γ-form of the peroxisome proliferator-activated receptors) may be implicated in ulcerative colitis. PPAR-γ receptor agonists have shown efficacy in ulcerative colitis and evidence has been accumulating that the mechanism of action of mesalazine may be mediated by PPAR-γ receptors.
Pharmacodynamic effects: The Mezavant XL tablet contains a core of mesalazine (5-aminosalicylic acid) 1.2g formulated in a multi-matrix system. This system is coated with Methacrylic Acid Copolymer, Type A and Methacrylic Acid Copolymer, Type B which are designed to delay release of mesalazine until exposure to approximately pH 7.
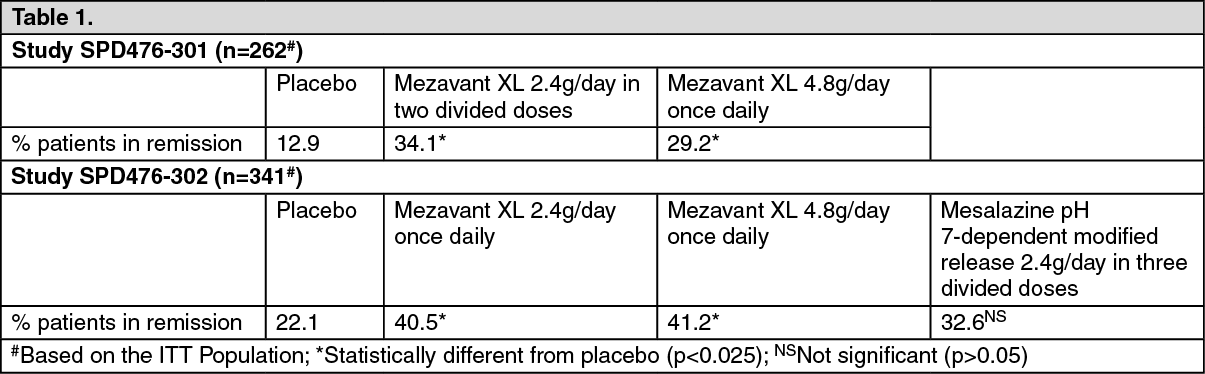
Clinical efficacy and safety: Mezavant XL was investigated in two similarly designed, Phase 3, placebo-controlled studies (SPD476-301 and SPD476-302) in 623 randomised patients with mild to moderate, active Ulcerative Colitis. Mezavant XL 2.4g/day and 4.8g/day administered with food achieved statistical superiority over placebo in terms of the number of patients achieving remission from Ulcerative Colitis after 8 weeks treatment. Using the Ulcerative Colitis Disease Activity Index (UC-DAI), remission was defined as a UC-DAI score of ≤1 with a score of 0 for rectal bleeding and stool frequency and at least a 1-point reduction in sigmoidoscopy score from baseline. Study SPD476-302, included a comparator, mesalazine pH 7-dependent modified release 2.4g/day (0.8g administered in 3 divided doses), as an internal reference arm. On the primary variable of remission, the following results were achieved: (See Table 1.)
 Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Pharmacokinetics: The mechanism of action of mesalazine (5-ASA) is not fully understood but appears to be topical, and therefore the clinical eficacy of Mezavant XL does not correlate with the pharmacokinetic profile. A major pathway of clearance of mesalazine is via metabolism to N-acetyl-5-aminosalicylic acid (Ac-5-ASA), which is pharmacologically inactive.
Absorption: Gamma-scintigraphy studies have shown that a single dose of Mezavant XL 1.2g passed rapidly and intact through the upper gastrointestinal tract of fasted healthy volunteers. Scintigraphic images showed a trail of radio-labelled tracer through the colon, indicating that mesalazine had spread throughout this region of the gastrointestinal tract. Complete disintegration of Mezavant XL and complete release of mesalazine occurred after approximately 17.4 hours.
The total absorption of mesalazine from Mezavant XL 2.4g or 4.8g given once daily for 14 days to healthy volunteers was found to be approximately 21-22% of the administered dose.
In a single dose study, Mezavant XL 1.2g, 2.4g and 4.8g were administered in the fasted state to healthy subjects. Plasma concentrations of mesalazine were detectable after 2 hours (median) and reached a maximum by 9-12 hours (median) on average for the doses studied. The pharmacokinetic parameters are highly variable among subjects. Mesalazine systemic exposure in terms of area under the plasma concentration-time curve (AUC) was dose proportional between 1.2g and 4.8g Mezavant XL. Maximum plasma concentrations (Cmax) of mesalazine increased approximately dose proportionately between 1.2g and 2.4g and less than dose proportional between 2.4g and 4.8g Mezavant XL, with the dose normalised value at 4.8g representing, on average, 74% of that at 2.4g based on geometric means.
In a single and multiple dose pharmacokinetic study of Mezavant XL 2.4 and 4.8g administered with standard meals in 56 healthy volunteers, plasma concentrations of mesalazine were detectable after 4 hours and were maximal by 8 hours after the single dose. At steady state (achieved generally by 2 days after dosing), 5-ASA accumulation was 1.1- to 1.4- fold for the 2.4g and 4.8g dose, respectively, above that expected on the basis of single dose pharmacokinetics.
Administration of a single dose of Mezavant XL 4.8g with a high fat meal resulted in further delay in absorption and mesalazine plasma levels were detectable after approximately 4 hours following dosing. However, a high fat meal increased systemic exposure of mesalazine (mean Cmax by 91%; mean AUC 16%) compared to results in the fasted state. Mezavant XL was administered with food in the Phase 3 trials.
In a single dose pharmacokinetic study of Mezavant XL, 4.8g was administered in the fasted state to 71 healthy male and female volunteers (28 young (18-35 yrs); 28 elderly (65-75 yrs); 15 elderly (>75 yrs)). Increased age resulted in increased systemic exposure (up to approximately 2-fold, based on AUC0-t, AUC0-∞ and Cmax) to mesalazine and its metabolite N-acetyl-5-aminosalicylic acid but did not affect the percentage of mesalazine absorbed. Increased age resulted in a slower apparent elimination of mesalazine, though there was high between-subject variability. Systemic exposures in individual subjects were inversely correlated with renal function as assessed by estimated creatinine clearance.
Distribution: Following dosing of Mezavant XL, the distribution profile of mesalazine is presumed to be the same as that of other mesalazine containing products. Mesalazine has a relatively small volume of distribution of approximately 18 L confirming minimal extravascular penetration of systemically available drug. Mesalazine is 43% bound and N-acetyl-5-aminosalicylic 78-83% bound to plasma proteins when in vitro plasma concentrations are up to 2.5 μg/mL and up to 10 μg/mL, respectively.
Biotransformation: The only major metabolite of mesalazine is N-acetyl-5-aminosalicylic acid, which is pharmacologically inactive. Its formation is brought about by N-acetyltransferase-1 (NAT-1) activity in the liver and in the cytosol of intestinal mucosal cells.
Elimination: Elimination of absorbed mesalazine is mainly via the renal route following metabolism to N-acetyl-5-aminosalicylic acid (acetylation). However, there is also limited excretion of the parent drug in urine. Of the approximately 21-22% of the dose absorbed, less than 8% of the dose was excreted unchanged in the urine at steady state after 24 hours, compared with greater than 13% for N-acetyl-5-aminosalicylic acid. The apparent terminal half-lives for mesalazine and its major metabolite after administration of Mezavant XL 2.4g and 4.8g were, on average, 7-9 hours and 8-12 hours, respectively.
Hepatic Impairment: There are no data in patients with hepatic impairment taking Mezavant XL. Systemic exposure to mesalazine increased by up to 2-fold in elderly subjects (>65 years, with a mean creatinine clearance of 68-76 mL/min) compared with younger adult subjects (18-35 years, mean creatinine clearance 124 mL/min) after a 4.8g single dose of Mezavant XL.
Renal impairment: Systemic exposures in individual subjects were inversely correlated with renal function as assessed by estimated creatinine clearance.
Elderly: The potential impact on the safe use of Mezavant XL in the elderly population in clinical practice should be considered. Furthermore, in patients with renal impairment, the resultant decrease in the rate of elimination and increased systemic concentration of mesalazine may constitute an increased risk of nephrotoxic adverse reactions (see Precautions).
In different clinical studies with Mezavant XL, mesalazine plasma AUC in females appeared up to 2-fold higher than in males.
Based on limited pharmacokinetic data, 5-ASA and Ac-5-ASA pharmacokinetics appear comparable between Caucasian and Hispanic subjects.
Pharmacokinetics data have not been investigated in elderly people.
Toxicology: Preclinical safety data: Effects in nonclinical studies were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
